




Hello and welcome to the Alcohol Alert, brought to you by The Institute of Alcohol Studies.
In this edition:
Marketing and Consumption of No and Low Alcohol Drinks – event recording
New way of calculating alcohol attributable deaths and hospital admissions 🎵 Podcast feature 🎵
Ireland introduces minimum unit pricing
World Heart Federation strongly rebukes ‘myth’ of alcohol prolonging life
Many schools use materials on alcohol harm from industry-funded sources
Heaviest drinkers bought 17 times the amount of alcohol as lowest drinkers in lockdowns
‘Misleading claims’ by industry in WHO consultation submissions
Children exposed to 554 brands every day, including from harmful commodities
Artificial Intelligence tech trialled to estimate age of customers
What language should we use and what language contributes to stigma?
We hope you enjoy our roundup of stories below: please feel free to share. Thank you.
IAS Blogs
To read blogs click here.
IAS Sustainability Series Seminar 4: Alcohol & Human Rights
The last seminar in our four-part series will consider human rights and alcohol, including:
Workers’ rights for alcohol industry employees in the developing world
Industry practices in Africa
Female promotional workers’ rights and their risk of sexual harassment and assault
Gender and health inequality
How human rights litigation can be used as a last resort control policy
You can watch the third seminar on YouTube where we discussed the alcohol industry’s sustainability commitments in the context of Corporate Social Responsibility activity.
Marketing and Consumption of No and Low Alcohol Drinks – event recording
On 27 January we held the launch of the findings of a new IAS-funded report by Dr Emily Nicholls of the University of York.
Dr Nicholls looked at whether there is potential for NoLos to support moderate drinking, whilst highlighting problematic marketing issues that reinforce harmful drinking and gender norms. The report will be launched end of February.
Catch up here:
New way of calculating alcohol attributable deaths and hospital admissions
🎵 Podcast feature 🎵
At the beginning of October, Public Health England (PHE) became the Office for Health Improvement and Disparities (OHID). One of their first jobs was to publish new estimates for alcohol attributable deaths and hospital admissions, due to an updated methodology and way of calculating these figures.
For alcohol-related conditions – conditions that are sometimes caused by alcohol but sometimes not – academics use what is called ‘alcohol attributable fractions’ (AAFs) to calculate the proportion of these cases caused by alcohol. As opposed to alcohol-specific conditions that are a direct consequence of alcohol use, which are far easier to work out.
AAFs are calculated by looking at the relative risk of certain diseases among those who drink compared to those who don’t drink, and the prevalence of alcohol consumption across the population.
AAF estimates were calculated in 2013 using the data PHE had at the time. Since then, drinking across the population has fallen on average and the relative risk has changed for 29 conditions. Therefore PHE/OHID recalculated using more up-to-date population figures.
The new calculation shows a 23% reduction in deaths and admissions, however as OHID says, this “doesn’t mean that the health risk due to alcohol is lower than it was before”. It means that people are drinking less across the population, but not that the risk of drinking has changed. Also worth noting is that the shocking 20% rise in alcohol-specific deaths last year remains unchanged.

Furthermore, this reduction in consumption seems to be happening among moderate drinkers, whereas heavier drinkers seem to be consuming more. Given heavier drinkers are more at risk of developing health conditions, this reduction across the adult population could be seen as a red herring.
Using the new method there are still almost 1 million alcohol-related hospital admissions in England each year.
Every few years the AAFs will need updating to reflect changes in consumption across the country.
Ireland introduces minimum unit pricing
The Republic of Ireland has commenced with its minimum unit pricing (MUP) policy, which sees the lowest price that can be charged for a gram of alcohol set at 10c, meaning a ‘standard drink’ — one that contains 10 grams of alcohol — will cost a minimum of €1. Here are some examples of the minimum products will now cost:

Table credit: Compton Solicitors
Ireland’s Minister for Health Stephen Donnelly said that “Addressing the availability of cheap strong alcohol products will reduce the disease and death caused by the harmful use of alcohol and will ensure that cheap strong alcohol is not available to children and young people at pocket money prices.”
As Alcohol Action Ireland explain on their website:
“MUP can save lives precisely because it targets only the strongest and cheapest drinks, which are the alcohol products favoured by two groups most vulnerable to alcohol-related harm – the very heaviest drinkers among us, who generally seek to get as much alcohol as they can for as little money as possible, and our young people, who generally have the least disposable income but the highest prevalence of binge drinking.
“MUP will have no impact on the price of a pint, or any alcohol sold in pubs, clubs or restaurants and will have little or no impact on those who drink in a low-risk manner.”
Alcohol producers and retailers are divided as to whether the measure is good news for them. The chief executive of the Convenience Stores and Newsagents Association said, “I represent retailers that are hard pushed at the moment, particularly as it’s so difficult to get staff and maintain them. They’ve been through a war and it’s given them a kick in the teeth by allowing this product to effectively be exported”. Some retailers have expressed concern that people living close to the border will drive to Northern Ireland to buy alcohol, where MUP is yet to be implemented. Many agree that the policy should be an all-island policy, to avoid such issues.
Eunan McKinney of Alcohol Action Ireland said:
“There is no question that introducing MUP to Northern Ireland, at the appropriate rate, would help reduce the dreadful impact of alcohol harm across the community. A renewal of a political commitment to the policy is now needed from all parties as Northern Ireland heads into the next electoral cycle.”
However, other retailers are less worried about any major financial impact, partly due to research from Scotland suggesting a “modest impact” on the drinks industry. For small producers and craft breweries that already sell products for a higher price, some argue it makes them more competitive with supermarkets and large multinational producers.
Professor Michel Destrade of NUI Galway was critical of the policy as he argues it will make alcohol retailers and illegal drug criminals richer: “Is it wise or correct for the Government to base an economic policy on the assumptions that price is enough to deter heavy drinkers and that heavy drinkers only seek cheap alcohol?”. Destrade argues that is likely that “heavy drinkers will switch to different beverage categories, cut down on other outgoings, travel more to Northern Ireland or France, support contraband, and switch to or increase their consumption of legal and illegal intoxicants”.
World Heart Federation strongly rebukes ‘myth’ of alcohol prolonging life
On Thursday 20 January the World Heart Federation (WHF) published a policy briefing that was widely covered in the media, which stated that:
“Risks due to alcohol consumption increase for all the major cardiovascular diseases, including hypertensive heart disease, cardiomyopathy, atrial fibrillation and flutter, and stroke. The widespread message for over 30 years from some researchers, the alcohol industry, and the media has been to promote the myth that alcohol prolongs life, chiefly by reducing the risk of CVD.”
They recommend that advocacy societies and organisations “must play a central role in advocating for stricter alcohol control measures… To begin with, all such actors should uniformly indicate that no level of alcohol is safe, given the current evidence”. Further, they argue that cardiology societies can play a role in a range of activity including advocating for WHO’s SAFER guidelines, calling for stricter regulation of alcohol, and for specific measures such as MUP.

Despite the WHF highlighting that the media and alcohol industry is somewhat to blame for this misinformation, a few papers sought comment from the trade body the Portman Group, who responded with: “It is important not to exaggerate the risk of moderate drinking and unduly alarm responsible consumers who are more than able to make informed decisions and enjoy alcohol sensibly”. On Twitter the Portman Group linked to another industry website which says, “the majority of large studies have found that risk [of CVD] is lower for individuals who are light or moderate drinkers than for those who do not drink at all”.
In response to this IAS released the following statement:
"The health risks of alcohol are in the news again today following the World Heart Federation (WHF) stating that “Risks due to alcohol consumption…. chiefly by reducing the risk of CVD [see above].”
“The evidence on the relationship between alcohol and cardiovascular diseases continues to accumulate, with reliable information available from Alcohol Change UK, Alcohol Focus Scotland, Alcohol Action Ireland, SHAAP and the WHF.
“Various media articles today sought comment from the alcohol industry on the WHF policy briefing, leading to industry organisations commenting on health matters. Research has shown alcohol industry and corporate social responsibility body funded materials may not be a reliable source of health information for the public. Health information on the risks of alcohol should be provided by independent bodies, free from conflicts of interest, just as the tobacco industry is not involved in educating about the risk of smoking."
Many schools use materials on alcohol harm from industry-funded sources
Research from the London School of Hygiene and Tropical Medicine was publish on 12 January which found that many schools use materials to educate children about alcohol harm that come from alcohol industry-funded sources.
The Guardian covered the story and said analysis by the researchers, including Dr May van Schalkwyk and Professor Mark Petticrew, found that the materials are potentially harmful because they downplay the harms drink can cause and seek to “blame-shift” responsibility for problems from manufacturers on to young people. They said:
“Alcohol industry-sponsored youth education programmes serve industry interests and promote moderate consumption while purportedly educating children about harms and influences of alcohol use.”
The materials they analysed are from Drinkaware, Smashed and Talk About Alcohol (a project by the Alcohol Education Trust) – all of which receive industry funding. Drinkaware swiftly removed the materials from their website and said: “The materials included in this research are out of date and don’t reflect our current guidance. They should have been removed from our website and they now have been. We’re sorry this didn’t happen sooner.”
Helena Conibear, the Alcohol Education Trust’s chief executive, accused the authors of “gross misrepresentation” and including “assertion”, “polemic” and selective quotation in their findings.
The publication found that the programmes promoted a familiarisation and normalisation of alcohol as a ‘normal’ adult consumer product, “which children must learn about and master how to use responsibly when older”.
The materials “employ selective presentation of harms, including misinformation about cancer”. Some misleadingly imply that only heavy or excessive drinking raises the risk of the disease.
Heaviest drinkers bought 17 times the amount of alcohol as lowest drinkers in lockdowns
A Newcastle University study was published on 19 January which analysed household purchasing data to understand the change in alcohol purchasing habits in Britain during the Covid lockdowns.
In a recent article the researchers stated that upon first review of the data there appeared to be a paradox; that despite the huge rise in alcohol harm and death in 2020, the amount of alcohol purchased remained relatively stable.
Their study looked at purchase data of 79,000 British households and found that the top fifth of households who previously bought the most alcohol increased their purchasing more than 17 times that of the lowest fifth that bought the least alcohol.

This contributes to evidence that suggests the 19% rise in alcohol-specific deaths in 2020 was due to heavier drinkers consuming more. As heavy drinkers are more at risk of alcohol harm, this increase in purchasing and consumption could have led to many being tipped over the edge into further harm and death.
The study also found that those living in the most disadvantaged households increased their purchases of alcohol more than those from the least disadvantaged households. Further, households with older residents and households in the north of England increased their purchases more than other groups.
Professor Sir Ian Gilmore of the Alcohol Health Alliance said:
“The pandemic highlights the urgent need for the Government to take action to protect the most vulnerable drinkers and disadvantaged communities from alcohol harm. This study suggests that minimum unit pricing can make a difference to purchases.”
The researchers concluded that:
“Alcohol policy to reduce high consumption of alcohol, and the availability of help and treatment to reduce alcohol consumption become more important during extraordinary times, such as COVID lockdowns.”
The study came out at the same time that The Royal College of Psychiatrists highlighted a big increase in the number of people drinking at ‘increasing or high risk’ levels. In the three months to the end of October 2021, 8 million people reported drinking at these levels, compared to 6 million up to February 2020, and 5 million up to October 2019.
Professor Julia Sinclair, the chair of the addictions faculty at the Royal College of Psychiatrists said:
“What we’re going to see is that some people who were perhaps drinking at a higher risk but weren’t physically dependent will have pushed themselves into being physically dependent, and they’re not the group who can suddenly wind back from this.”
The NHS also released alcohol statistics at the end of the month, which show there were 976,429 hospital admissions in 2019/20 linked to alcohol – a 16% rise from the previous data collected in 2016/17 – which makes up 5.7% of all hospital admissions in England.
They also highlighted the rising affordability of alcohol, which leads to increased alcohol harm, to which Dr Alison Giles was quoted by the Telegraph:
“The statistics highlight the false economy of the Government’s repeated cuts and freezes to alcohol duty in recent years, which will cumulatively cost the Treasury over £16.2 billion from 2013-2027, and further increase hospital admissions and death. This increasing affordability needs to be tackled, such as with a duty ‘escalator’ where alcohol duty rises with inflation each year, a policy that could form part of an alcohol strategy.”
‘Misleading claims’ by industry in WHO consultation submissions
The Centre for Alcohol Policy Research in Australia, supported by the Foundation for Alcohol Research and Education (FARE), has released a new report that shows alcohol companies and their lobby groups made 60 submissions to the World Health Organization’s consultation on its alcohol action plan, with many containing misleading claims and misrepresented scientific evidence”.
One of the main industry demands is to abandon what they label a “problematic” 2030 target of reducing consumption by 20% and instead to focus on reducing “harmful” consumption – a call that researchers and alcohol control advocates deem to be less effective due to its vagueness.
90% of the industry submissions called for greater alcohol company involvement in harm reduction and policy making and over 50% cast doubt on WHO’s evidence-based policies. Only 36% referenced any specific evidence to support their arguments, with most promoting weak evidence or misinterpreting it.
FARE’s Chief Cxecutive Caterina Giorgi said alcohol companies had been lobbying for decades to “minimise health concerns and delay effective measures” to reduce alcohol’s health impacts and they should have “no role in the development of health policy”.
ABA president Andrew Wilsmore said the industry has a legitimate role to play in policies that affect them, “to ensure that those policies are effective, efficient and grounded in reality”. Wilsmore said “We focus on supporting effective programs that focus on education, awareness and changing behaviours relating to alcohol consumption”.
Such measures have been repeatedly denounced by public health experts as ineffective, especially compared to evidence-based policies advocated for by the WHO. In 2017 Professor Mark Petticrew wrote that “the argument against the implementation of effective population-level measures appears to be constructed from at least five frequently recurring elements” including “claims that information, education and personal responsibility are the appropriate and/or most effective solutions”.
Artificial Intelligence tech trialled to estimate age of customers
Five major supermarkets will be trialling facial age estimation technology between January and May this year, via self-service terminals.
The technology – Yoti – will take photos of consenting customers who have alcohol in their basket and will estimate their age. The tech claims to have an average accuracy of within 2.2 years for all ages, and within 1.5 years for people aged 16-20 years old. The machine will delete the photos after estimation. During the trial customers will still be required to present ID if asked.
The trial is part of the Government’s ‘regulatory sandbox’, which looks to test ways to “improve the experience of consumers and retailers when purchasing age restricted products”.
At the end of 2021 IAS published a report developed by Jessica Muirhead of Wrexham Glyndŵr University on ‘Preventing underage alcohol purchasing online using payment card details’, which the Government is looking at as an option.
Children exposed to 554 brands every day, including from harmful commodities
A New Zealand study that placed wearable cameras on 90 children aged 11-13 found that they were exposed to a mean average of 554 brands per 10 hour day, almost a brand every minute.
The brands were seen predominantly as product labels (36% of exposures) and product packaging (22%), and mostly in school (43%) and at home (30%).
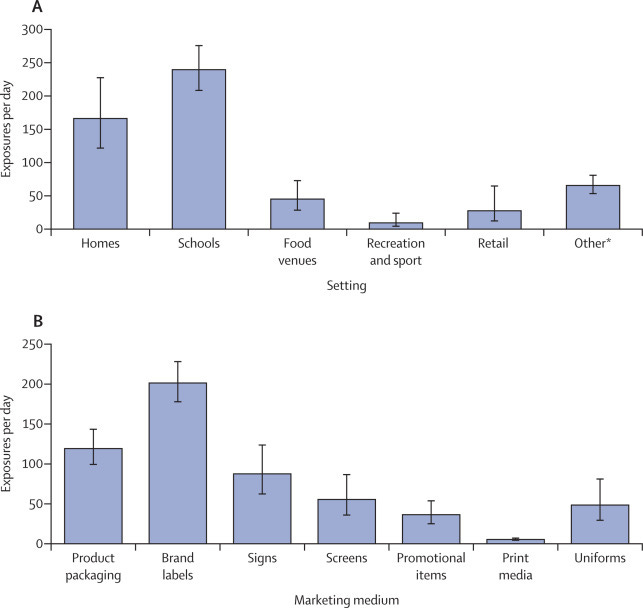
Food and beverages were the dominant product category with 20% of exposures and the most pervasive marketing brands typically sold a range of products across more than one product category. For instance children were exposed to Nike on average 20 times per day.
Children were exposed to more than twice as many harmful commodities as core food and social marketing messages (76 compared to 32 per 10hr day). Harmful commodities included junk food, alcohol and gambling.
The researchers concluded that:
“Given the key role marketing plays in establishing and supporting consumption norms, and perpetuating the normalisation of overconsumption which contributes to environmental degradation, these findings suggest an urgent need to reduce marketing to promote planetary health.”
What language should we use and what language contributes to stigma?
Dr Kristen Fuller writes that our brain responds to words with a process we call “associative activation”, where after hearing a word we form an idea followed by an emotion which then produces an action or reaction.
She says that as a result, words have “an immediate, visceral adverse reaction. When we hear words like “crazy,” “addict,” or “alcoholic,” we immediately label the individual as bad, simply because of the stigmatising language that our brain processes into a visceral negative emotion”.
Dr Fuller writes that reframing terms to be more “person-centred” means we don’t define people by their illness e.g. instead of calling someone “mentally ill” say “a person living with a mental health condition”, or “a person living with an alcohol use disorder” instead of “an alcoholic”.
Alcohol Change UK (ACUK) has an excellent briefing on its website which discusses how we should talk about alcohol.
ACUK is currently working with the University of Stirling on a project that will look at how we frame alcohol harm.
The UK Alcohol Alert (incorporating Alliance News) is designed and produced by The Institute of Alcohol Studies. Please click the image below to visit our website and find out more about us and what we do, or the ‘Contact us’ button. Thank you.









